Postgraduate Training Course in Reproductive Health 2004
Balanced protein energy supplementation during pregnancy
for the prevention of IUGR
Review of the literature based on the Cochrane Library systematic review of balanced protein energy supplementation in pregnancy
Nadine Alaa Sherif
Lecturer of Obstetrics and Gynaecology
Faculty of Medicine, Cairo University
See also
![]() presentation
presentation
Background
Low birth weight (LBW) is an important problem in public health, as it is associated with increased neonatal mortality. Fifty percent of the 3.9 million neonatal deaths per year are due to babies born too small either because of intrauterine growth restriction (IUGR) or preterm delivery. In developing countries low birth weight babies are more likely to be due to IUGR than in developed countries, so in developing countries IUGR is an important determinant of perinatal mortality. Morbidity is also increased in low birth weight newborns and the negative effects of IUGR tend to persist in infancy as deficits in growth and neurological development. There is evidence that the negative effects of IUGR could persist long after infancy as low birth weight has been associated with the development of cardiovascular disease, high blood pressure, obstructive lung disease, diabetes, high cholesterol and renal damage in adulthood. Imbalances in maternal nutrition can adversely affect normal fetal growth and development, so preventing maternal malnutrition could decrease the risk of IUGR. Among all nutritional interventions for the prevention of IUGR, protein energy supplementation appears to be the most promising one as shown by a systematic review published in the Cochrane Library.
Therefore the objectives of this paper were:
- To review the trials which have tested protein energy supplementation as a preventive strategy for IUGR
- To describe what are the public health implications of the results of those studies with their possible emphasis on the reality in Egypt
These objectives have been achieved by:
- reviewing 13 trials included in the Cochrane review
- identifying new trials if published
- discussing the implications of these results
This area of research is important because maternal nutrition as related to IUGR is a public health problem worldwide. Nutritional interventions are relatively cheap and can be implemented in large populations contributing to decrease the problem of IUGR and perinatal mortality
Methodology
We have assessed the reports of randomized clinical trails included in
the Cochrane systematic review of balanced protein energy supplementation
in pregnancy. The systematic review included 13 studies. We have focused
on the outcome ‘small for gestational age’ as a proxy for IUGR. Six trials
reported Small for gestational age as an outcome, thus we considered those
trials for the purpose of this paper.
Data from the systematic review were discussed together with data of LBW
among Egyptian infants given by the Egyptian National Perinatal Care Program
(ENPCP) taken from 80 neonatology units in different hospitals, and from
the data given by the Egyptian Demographic Health Survey (EDHS) in 1995
and 2000, and from the data of the Ministry of Health and Population (MOHP).
Finally recommendations were given after the analysis of all the previous data mentioned before.
Results
Table 1 shows the characteristics of the six trials included in
the systematic review and reported small for gestational age as an outcome.
The trials were different in terms of time of the study, population studied,
sample size, type and amount of supplementation: 4 trials were from underprivileged
areas from developing countries (Taiwan, India, Columbia, and the Gambia)
while 2 were from Wales and Harlem. The method of supplementation was also
different: Blackwell used 40g protein and 800kcal energy, Mora 38.4g protein
and 865kcal energy, Rush used 6g protein and 322kcal energy, Elwood supplemented
with fat free milk, Girija supplemented with 30g protein and 417kcal energy
and Ceesay used supplementation of 22g protein and 1.017kcal.
Table 1: Characteristics of included studies:
| Author | Country | Population characteristics | Intervention |
| Blackwell 1973 | Taiwan | 182 well-nourished Taiwanese women with marginal diets (estimated daily protein intake</=40g | Supplemented: Pre-pregnancy and pregnancy
supplement containing 40g protein and 800kcal energy plus vitamins
and minerals Controls: supplement containing vitamins and minerals only |
| Ceesay 1997 | Gambia | 2047 rural Gambian women from 28 villages with chronically marginal nutrition. Malnutrition more pronounced from June to October (the hungry season involving low food supply and heavy agricultural work) than from November to May (the dry harvest season with adequate food supply and less strenuous work) | Supplemented: Two supplement biscuits
containing 4250kj (1.017 kcal) energy, 22g protein, 56g fat, 47mg
calcium, and 1.8mg iron consumed daily in presence of birth attendants.
Supplementation began at 20 weeks gestation Control villages: no supplement |
| Elwood 1981 | Wales | 1153 adequately-nourished pregnant women in two small Welsh towns recruited at time of first reporting of pregnancy | Supplemented: fat free milk Control: no intervention |
| Girija 1984 | India | 20 poor Indian women during the last trimester | Supplemented: supplement containing
417Kcal energy and 30g protein Control: normal (unsupplemented)diet |
| Mora 1978 | Bogota; Columbia | 339 undernourished poor women in the first or second trimester for Bogota slum for whom at least 50%of previous children had weight to height<85%of Columbia standard | Supplemented: supplement containing
865kcal energy and 38.4g protein beginning in third trimester Control: normal (unsupplemented) diet |
| Rush 1980 | Harlem; New York; USA | 529 low income black women in Harlem (New York City) at risk for low birth weight based on one or more of the following criteria: pre-pregnancy weight<110Ibs, pre-pregnancy weight 110-139Ibs plus low gestational weight gain as of recruitment; pre-pregnancy weight 110-139Ibs plus previous history of low birth weight, or pregnancy weight 110-130Ibs plus protein intake<50grams in the 24hours preceding registration | Supplemented: supplement containing
322kcal energy, 6g protein, and vitamins/minerals (complement) Control: supplement containing vitamins/minerals only |
Table 2 shows the results of the systematic review of clinical trials of protein energy supplementation in pregnancy. There was a decreased incidence of SGA by nearly 30% as shown by a relative risk (RR) of 0.68. The estimated RR in each trial ranged from 0.88 to 0.09 showing homogeneity in the direction of the results but variation in the magnitude of the effect. Also, the much higher energy supplement provided in the Gambian trial (Ceesay 1997) appeared to have a much larger effect on fetal growth.
Table 2: Results of the systematic review of clinical trials of protein energy supplementation in pregnancy
| Study | Supplemented | No SGA | Control | No SGA | RR | 95% CI |
| Blackwell 1973 | 94 | 6 | 88 | 10 | 0.56 | 0.21-1.48 |
| Ceesay 1997 | 1010 | 112 | 1037 | 176 | 0.65 | 0.56-0.81 |
| Elwood 1997 | 591 | 25 | 562 | 27 | 0.88 | 0.52-1.50 |
| Girija 1984 | 10 | 0 | 10 | 5 | 0.09 | 0.01-1.45 |
| Mora 1978 | 177 | 12 | 162 | 14 | 0.78 | 0.37-1.65 |
| Rush 1980 | 265 | 30 | 264 | 43 | 0.70 | 0.45-1.07 |
| Total | 2147 | 185 | 2123 | 275 | 0.68 | 0.57-0.80 |
Discussion
Protein energy supplementations appear to be a promising public health intervention for the prevention of IUGR. The studies examined were conducted in different populations, which increase the generalizability of the results and show that protein energy supplementation decreased the risk of IUGR overall by 30%, being an important result for a single nutritional intervention.
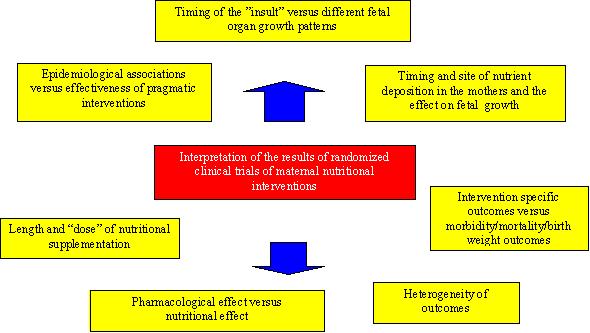
When examining results of clinical trials of nutritional supplementation in pregnancy, it has been suggested that the interpretation of the results should take into consideration several factors that can be examined in a conceptual framework. This is particularly important when one has to decide on the practical implications of positive and negative results from clinical trials. Figure 1 presents a framework, as proposed by Villar (Villar 2003), and suggests several topics for discussion.
Epidemiological association versus effectiveness of pragmatic interventions
A large proportion of epidemiological evidence supports the association
between protein energy malnutrition before or during pregnancy and low fetal
birth weight. It is important to differentiate the practical implications
of these epidemiological associations from the effectiveness of pragmatic
interventions during the reproductive period (Villar 1996). Even if the
randomization process in clinical trials reduces the effect of confounding
variables on the results, one should still consider that infections and
other conditions may play a role for IUGR, and that these conditions may
be more prevalent in populations other than the ones studied.
Timing of the insult and different fetal organ growth patterns
The effect of protein energy malnutrition or of any other nutritional intervention
is very likely to be related to the timing of occurrence during gestation.
This is partially due to the differential fetal organ growth patterns (Villar
1982) (e.g. as shown by ultrasonography and magnetic resonance imaging of
the brain, liver, colon, biparietal diameter and femur length). Thus, nutritional
deficiencies and suplementation can have different effects on fetal growth
depending on the time of occurrence during pregnancy. When implementing
intervention shown to be effective one has to take into account when during
pregnancy it will be most effective to intervene.
Timing of nutrient deposition in the mother and the effect on fetal
growth
Differential timing of nutrient deposition (weight gain during pregnancy)
and its body location may also influence nutrient transfer to the fetus
and therefore the effect of nutritional interventions during pregnancy.
Patterns of fat and fat-free mass deposition differ in terms of location
(e.g., thigh and sub scapular versus triceps skinfold) and timing (first
and second trimester versus third trimester) (Villar 1992). Birth weight
is associated more with maternal changes in thigh skinfolds and early fat
gain than with other body sites or pregnancy timing (Mardones-Santander
1998). This is another factor to consider when explaining variability in
the results of clinical trials and planning related interventions.
Length and amount of nutritional supplementation
The concept of timing includes the length of supplementation and amount
because it is unrealistic that chronic malnutrition during two or three
decades of life will be overcome with only a few months of extra nutrient
intake. As an example, it has been shown that energy supplementation had
a biologically substantive effect when it was provided to women during two
consecutive pregnancies and during lactation period but a modest effect
when women were supplemented only during the index gestation (Villar 1988)
Pharmacological effect versus nutritional effect
A harmful effect may be obtained if supplementation is given to individuals
with an adequate nutritional intake. This was shown in a trial that
provided pregnant women without protein deficiency with a high-protein supplement
(Rush 1980). This pharmacological intervention had a negative effect on
the rates of small for gestational age and infants born to supplemented
mothers had lower birth weight.
Intervention-specific outcomes versus overall outcomes for fetal growth
and birth weight
Identifying the primary outcome or the most specific outcome in reference
to the protein energy malnutrition is a key element. Maternal underweight
may not be associated with pregnancy complications such as preeclampsia,
gestational diabetes, placenta praevia or abruptio placentae, yet underweight
mothers have been shown to be at higher risk for having newborns with birth
weight below the 5th percentile and preterm delivery (Sebire 2001). Similarly,
birth weight could be a too crude outcome to detect all the possible effects
of maternal nutritional supplementation. Other components of growth, such
as bone growth and soft tissue growth, could be evaluated to obtain more
information on the effects of nutritional supplementation on fetal growth.
We should also address the question of the relative importance of the long
term outcomes of perinatal nutritional interventions. The relationship between
fetal nutrition and adult disease (Godfrey 2000,Joseph 1996) are still being
debated; there is limited evidence from randomized controlled trials(Singhal
2001)
Heterogeneity of outcomes
In evaluating the effect of nutritional intervention on pregnancy outcomes,
it is important to emphasize the heterogeneous nature of the outcomes considered.
For example, not all low birth weight infants are the same (preterm vs IUGR)
(Kramer, 1987) and not all LBW result from the same cause (e g. it may be
due to preeclampsia or protein energy malnutrition). Therefore, it is unlikely
that nutritional supplementation provided to all women with LBW babies (some
may not even have nutritional deficiencies) will have a major effect in
preventing IUGR overall.
Taking into consideration the conceptual framework, the results of the systematic review have important implication for future practice and research.
Implications for practice
The positive effect of balanced protein energy supplementation on impaired fetal growth suggests that this might be the only nutritional intervention for which a practical recommendation can be made. Kramer (Kramer 2001) suggested that balanced protein energy supplementation should be provided to all women in areas with a high prevalence of maternal malnutrition rather than only to women considered at risk of malnutrition on the basis of anthropometric screening.
Implications for research
Future studies are needed to evaluate the effect of pre-conceptional, peri-conceptional and prenatal micronutrient supplementation in addition to protein energy supplementation on fetal size at birth. Multiple supplementations may increase the positive effect observed with protein energy supplementation alone. Also, it will be critical to study the mechanism of action of different nutrients on organ growth and placental circulation. Future studies should also extend the follow up of infants to childhood and possibly adulthood to determine the biological importance of more specific outcomes of fetal growth, such as bone or soft tissue growth that now can be assessed by ultrasonography. These implications are important for a country like Egypt, where 50% of all LBW babies can be attributed to IUGR. The prevalence of low birth weight is higher in mothers of low socio-economic class who are more likely to be malnourished. In a study from the Egyptian National Perinatal Care Program (ENPCP) in 80 hospital neonatology units in the MOHP, a negative correlation between neonatal mortality and birth weight was reported. Mortality rate was high among very low birth weight neonates (VLBW<1500g) reaching 56.5%, while it was 25.1% among LBW<2500-1500g. Furthermore, mortality rate was also high among normal birth weight neonates (>2500g) admitted to the neonatology units, as it reached 12.5%. The study also found a large proportion of LBW neonates were born full term, therefore being SGA or IUGR. These findings confirmed the need for prevention and early detection of IUGR, and of hospital care for both term and premature neonates (Mansour 1998a, LBWSE 2000). In this respect, the risk approach, which is an integral part of an organised perinatal health care delivery, postulate the use of obstetric risk screening or scoring systems to predict neonates at risk of IUGR or prematurity to be targeted for care. This method has proven to be an effective policy to reduce mortality and morbidity (Backett 1984, Barlett 1993) and could be complemented by appropriate nutritional interventions.
References
- Afia AA, Fouad S, Hasanein A (1999): Small for gestational age neonates, prevalence and etiologic study. Al Azhar J Pediatr; 2 (1): 69-75.
- Backett EM, Davis AM, Petros-Barvazian A. The risk approach in health care. With special reference to maternal and child health, including family planning. Public Health Pap. 1984;76:1-113. [PubMed]
- Barlett AIII, Paz de Bocaletti MA (1993): Reducing perinatal mortality in developing countries: High risk or improved labour management? Health Policy and Planning. 8 (4): 360-368.
- Low Birth Weight Study in Egypt (LBWSE), 1995-1997. Ministry of Health and Population, Health Mother Child Project in Collaboration with USAID, 2000
- Mansour E, Eissa A, Little G (1998a): Screening of cases admitted in 80 neonatal units in ministry of health hospitals during the period January 95- June 96. Egyptian J Pediatr. 15 (1&2): 173-182.
- Villar J, Merialdi M, Gulmezoglu M, Abalos E, Carroli G, Kulier R, de Onis M. Characteristics of randomized controlled trials included in systematic reviews of nutritional interventions reporting maternal morbidity, mortality, preterm delivery, intrauterine growth restriction and small for gestational age and birth weight outcomes. J Nutr. 2003 May;133(5 Suppl 2):1632S-1639S [PubMed]
- Villar J, Carroli G. Methodological issues of randomized controlled trials for the evaluation of the reproductive health interventions. Prev Med. 1996 May-Jun;25(3):365-75 [PubMed]
- Villar J, Belizan JM. The timing factor in the pathophysiology of the intrauterine growth retardation syndrome. Obstet Gynecol Surv. 1982 Aug;37(8):499-506 [PubMed]
- Garden AS, Roberts N. Fetal and fetal organ volume estimations with magnetic resonance imaging. Am J Obstet Gynecol. 1996 Aug;175(2):442-8 [PubMed]
- Harding JE. The nutritional basis of the fetal origins of adult disease. Int J Epidemiol. 2001 Feb;30(1):15-23.[PubMed]
- Cuttini M, Cortinovis I, Bossi A and de Vonderweid U. Proportionality of small for gestational age babies as a predictor of neonatal mortality and morbidity. Paediatr Perinat Epidemiol. 1991 Jan;5(1):56-63[PubMed]
- Villar J, Cogswell M, Kestler E, Castillo P, Menendez R, Repke JT. Effect of fat and fat-free mass deposition during pregnancy on birth weight. Am J Obstet Gynecol. 1992 Nov;167(5):1344-52. [PubMed]
- Mardones-Santander F, Salazar G, Rosso P, Villarroel L. Maternal body composition near term and birth weight. Obstet Gynecol. 1998 Jun;91(6):873-7.[PubMed]
- Villar J, Rivera J. Nutritional supplementation during two consecutive pregnancies and the interim lactation period: effect on birth weight. Pediatrics. 1988 Jan;81(1):51-7. [PubMed]
- Rush D, Stein Z, Susser M. Controlled trial of prenatal nutrition supplementation defended. Pediatrics. 1980 Oct;66(4):656-8. [PubMed]
- Kramer MS. Determinants of low birth weight: methodological assessment and meta-analysis. Bull World Health Organ. 1987;65(5):663-737.[PubMed
- Goldenberg RL, Rouse DJ. Prevention of premature birth. N Engl J Med. 1998 Jul 30;339(5):313-20. Review [PubMed
- Roberts J (2002): President`s welcome. Hypertens. Pregnancy 21: vii-viii
- Gulmezoglu M, Villar J, Hofmeyer J, Duley L, Belizan JM. Randomised trials in maternal and perinatal medicine: global partnerships are the way forward. Br J Obstet Gynaecol. 1998 Dec;105(12):1244-7 [Abstract]
- Global Forum for Health Research and WHO (2002): Child Health Research - a foundation for improving child health. Geneva: World Health Organization, WHO/FCH/CAH/02.3. [Link]
- de Onis M (2001): Intrauterine growth retardation. 2020 Vision Focus, (Brief 5), 2001. Editors: Rafael Flores and Stuart Gillespie: Washington, DC: International Food Policy Research Institute
- Robert E (1999): Reducing perinatal and neonatal mortality. Report of a meeting, Baltimore, May 10-12
- Merialdi M, Carroli G, Villar J, Abalos E, Gulmezoglu AM, Kulier R, De Onis M. Nutritional interventions during pregnancy for the prevention or treatment of impaired fetal growth: an overview of randomized controlled trials. J Nutr. 2003 May;133(5 Suppl 2):1626S-1631S. [PubMed]
- Fall CH, Yajnik CS, Rao S, Davies AA, Brown N, Farrant HJ. Micronutrients and fetal growth. J Nutr. 2003 May;133(5 Suppl 2):1747S-1756S [PubMed
- Kramer MS. Isocaloric balanced protein supplementation in pregnancy. Cochrane Database Syst Rev. 2000;(2):CD000118.[PubMed]
- Duley L, Henderson-Smart DJ. Drugs for treatment of very high blood pressure during pregnancy. Cochrane Database Syst Rev. 2002;(4):CD001449 [PubMed]
- Atallah AN, Hofmeyr GJ, Duley L. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev. 2002;(1):CD001059. [PubMed]
- Mahomed K . Iron and folate supplementation in pregnancy. Cochrane Database Syst Rev. 2000;(2):CD001135. [PubMed]
- Merialdi M (2003): Low Birth Weight Infants: Causes, Prevalence and Prevention (personal communication)
- Deter RL, Harrist RB (1993): Assessment of normal fetal growth. In: Ultrasound in Obstetrics and Gynecology ( Chervenak, F. A., Isaacson, G. C., and Campbell, S., eds), pp. 361-385. Little, Brown and Company, Boston/ Torento/ London.
- Deter RL, Harrist RB, Hadlock FP, Carpenter RJ. Fetal head and abdominal circumferences: I. Evaluation of measurement errors. J Clin Ultrasound. 1982 Oct;10(8):357-63. [PubMed]
- Kramp E, Lees C, Bland, JM, Espinoza DJ, Moscoso G, Campbell, S (2000): Fetal biometry at 4300m compared to sea level in Peru. Ultrasound Obstet Gynecol 16: 9-18.
- Blackwell RQ, Chow BF, Chinn KSK, Blackwell BN, Hsu SC (1973): Prospective maternal nutrition study in Taiwan: rationale, study design, feasibility and preliminary findings. Nutrition Reports International 1973; 7: 517- 32
- Ceesay SM, Prentice AM, Cole TJ, Foord F, Weaver LT, Poskitt EM, Whitehead RG. Effects on birth weight and perinatal mortality of maternal dietary supplements in rural Gambia: 5 year randomised controlled trial . BMJ. 1997 Sep 27;315(7111):786-90. [PubMed
- Elwood PC, Haley TJ, Hughes SJ, Sweetnam PM, Gray OP, Davies DP. Child growth (0-5 years), and the effect of entitlement to a milk supplement. Arch Dis Child. 1981 Nov;56(11):831-5 [PubMed]
- Girija A, Geervani P, Rao GN. Influence of dietary supplementation during pregnancy on lactation performance. J Trop Pediatr. 1984 Apr;30(2):79-83.[PubMed]
- Mora JO, Clement J, Christiansen N, Suescun J, Wagner M, Herrera MG (1978): Nutritional supplementation and the outcome of pregnancy. III Perinatal and neonatal mortality. Nutrition Reports International; 18: 167-75
- Sebire NJ, Jolly M, Harris JP, Wadsworth J, Joffe M, Beard RW, Regan L, Robinson S. Is maternal underweight really a risk factor for adverse pregnancy outcome? A population-based study in London. BJOG. 2001 Jan;108(1):61-6. [PubMed]
- Godfrey KM, Barker DJ. Fetal nutrition and adult disease. Am J Clin Nutr. 2000 May;71(5 Suppl):1344S-52S.[PubMed]
- Joseph KS, Kramer MS. Review of the evidence on fetal and early childhood antecedents of adult chronic disease. Epidemiol Rev. 1996;18(2):158-74. [PubMed]
- Singhal A, Cole TJ, Lucas A . Early nutrition in preterm infants and later blood pressure: two cohorts after randomised trials. Lancet. 2001 Feb 10;357(9254):413-9.[PubMed]
- Kramer MS, Victoria CG (2001): Low birth weight and perinatal mortality. In : Nutrition and Health in Developing Countries (Semba, RD and Bloem MW, eds), pp. 57-70. Humana Press, Totowa, NJ.