First Consensus Meeting on Menopause in the East Asian Region
Demography of the menopause and pattern of climacteric symptoms in the East Asian region
Takeshi Aso
Department of Obstetrics and Gynaecology, Tokyo Medical and Dental University School of Medicine, Tokyo, Japan
Introduction
The onset of the menopause not only signals the end of a woman’s reproductive function but also the start of a new phase in which she has the freedom to appreciate the quality of her life. A woman’s physical and mental condition during this stage of her life will have a significant influence on her later years.
The concept of the menopause encompasses a number of factors which can vary from country to country according to tradition, culture and socioeconomic conditions. In the East Asian region in particular, the factors in each country and area vary tremendously. In order to understand both the specific advantages and disadvantages in the management of the menopause in each part of this region, it is important to discuss the demography of population growth and mortality. It is also necessary to evaluate the climacteric symptoms which are common or specific to perimenopausal women in each country. The overview resulting from a constructive discussion of these issues should have a significant impact on improving the quality of life of menopausal women throughout the world.
Background to the East Asian region
In the 1996 World Health Report [1], South-East Asia and the Western Pacific are included in those regions corresponding to East Asia. Ten countries belonging to South-East Asia and 27 countries in the Western Pacific have populations of 1.4 and 1.6 billion, respectively. These countries are spread throughout a wide area and cover extremely heterogeneous ethnic backgrounds, cultures, economies, social structures and epidemiological characteristics. According to the United Nations classification, for analytical purposes most of these countries are termed developing countries. Up to the present, it has been difficult to collect reliable statistics covering population growth, mortality and menopausal status in these countries. The overview given in this paper has been compiled mainly from the available reports and communications of 15 countries in this region, namely, Cambodia, China, Democratic People’s Republic of Korea, Hong Kong, Indonesia, Japan, Laos, Malaysia, Mongolia, Myanmar, Philippines, Republic of Korea, Singapore, Thailand and Vietnam.
Proportion of postmenopausal women in the population
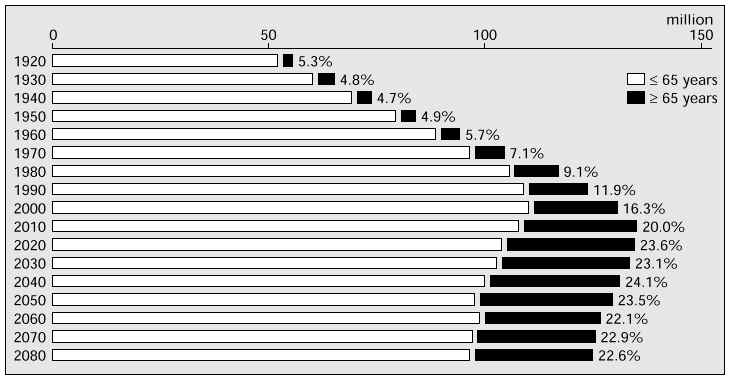
In 1990, the total population of postmenopausal women throughout the world was reported to number 476 million. An analysis of the distribution of postmenopausal women revealed that 40% live in the industrialized world. It is predicted that the total number of postmenopausal women in 2030 will be approximately 1200 million and the proportion of those living in the developing world will increase to 76% [2]. The available data from 1989 to 1992 postulated that the percentages of the population above 45 years of age in the 11 countries (except Japan) in the East Asian region ranged from 15.3 to 24.0%, and those above 65 ranged from 3.8 to 6.6% [3]. In Japan, as shown in Figure 1, the proportion of the population above 65 years of age in 1995 was 14.5% and the male:female ratio was 2:3. It is projected that the proportion will increase up to 27% in 2025 [4]. The population projections for China given in the 1993 World Development Report [2] indicate that the proportion of women aged 50 and over to the total population in 1990 was 8.20% and that in 2010 and 2030 it will be 11.28 and 17.08%, respectively. These figures suggest sharp increases in the proportion of postmenopausal women over the next 20–30 years in these two countries.
Fig. 1: The proportion of the population aged 65 years and over to the total population in Japan from 1920 to 2080.
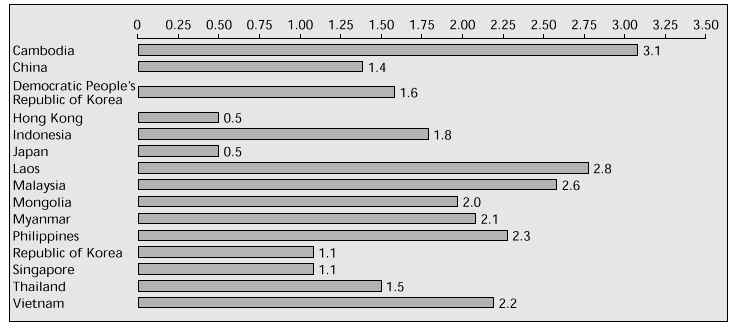
The total fertility rates of the 12 countries in 1995 are shown in Figure 2 [5]. The rates of seven of these countries were greater than 2.0. Figure 3 shows the annual growth rates of the total population in 1995 based on these and additional data [5]. The rates of two countries, Hong Kong and Japan, are 0.5. Estimated life expectancies at birth in 1995 are shown in Figure 4 [5]. In every country, women have a greater life expectancy than men. Although the limitation of reliable statistics in most of the countries in the East Asian region makes it difficult to obtain a precise projection, the rate of increase in the number of postmenopausal women is suggested to be accelerated in this part of the world. Taking together these local changes in life expectancy at birth and the global trend, it is strongly indicated that the future postmenopausal population will increase dramatically in the developing world, more so than in the industrialized world.
Fig. 2: Total fertility rates in 1995 of 12 countries in the East Asian region (%).
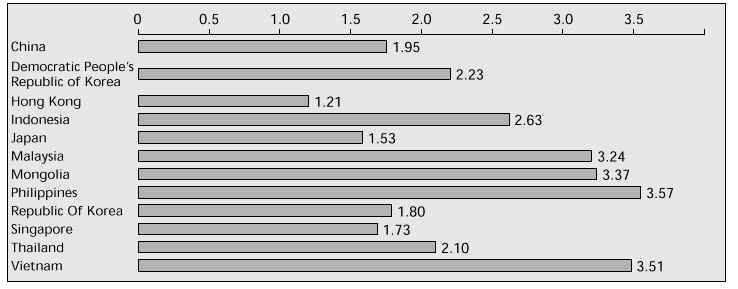
Fig. 3: Annual growth rates of the total population in 1995 of the East Asian region (%).
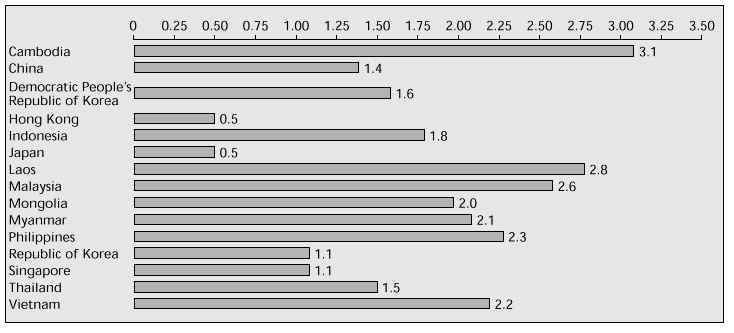
Fig. 4: Life expectancy at birth in 1995 of 12 countries in the East Asian region (years).
Mortality of postmenopausal women
Women in their reproductive years are protected from the risks of cardiovascular disease mainly because of the beneficial effects of the ovarian hormone, oestrogen. Once their oestrogen levels decrease following the menopause, the risk of mortality from cardiovascular disease rises to the level of that in men. On the other hand, female mortality rates from malignant neoplasms are higher during the reproductive period than during the postmenopausal years. The overall mortality rates of women are lower than those of men throughout the reproductive period, but they increase after the menopause. Such differences in mortality between men and women, as well as between pre- and postmenopause, have been documented in studies mostly based on US and European populations.
In general, the majority of countries in the East Asian region are in the early stages of an epidemiological transition (the changing pattern of mortality and morbidity in association with demographic changes) in mortality. In some countries, infectious diseases are gradually being replaced by non-infectious and non-communicable conditions such as cardiovascular disease, cancer, congenital anomalies, endocrine disorders and accidents. Data concerning the current mortality of postmenopausal women have not been fully surveyed in the majority of countries in this region.
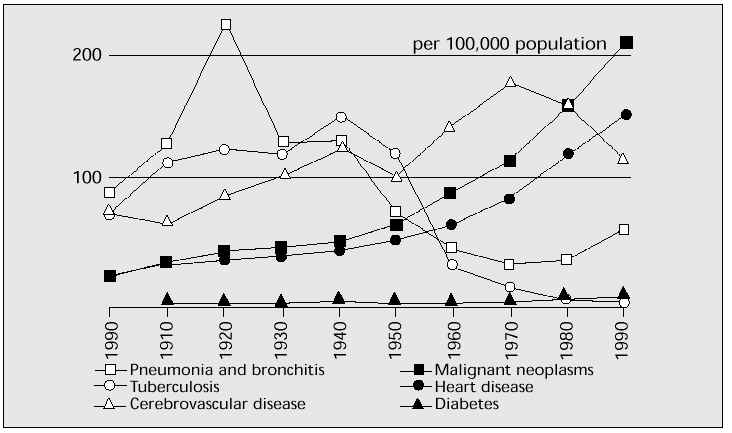
However, an analysis of the changes in mortality during recent decades in Japan (which has adequate statistics) may have some predictive value in estimating the future situation in the East Asian region as a whole [6]. The main reason for the decline in overall mortality in the last 50 years in Japan has been the decrease in mortality from infectious diseases such as pneumonia, bronchitis and tuberculosis. By contrast, the mortality rate from cerebrovascular disease has increased slightly, and that from heart disease and malignant neoplasms has increased markedly in the last 30 years (Fig. 5). The sharp decrease in mortality from infectious diseases is attributable to the improvement in living standards, whereas the increase in deaths from so-called adult diseases including malignant neoplasms, cardiovascular disease, cerebrovascular disease and diabetes mellitus is partly explained by the changes in diet and other life style factors, and partly by the increasing proportion of elderly in the total population.
Fig. 5: The change in mortality rates from major diseases during the past 90 years in Japan.
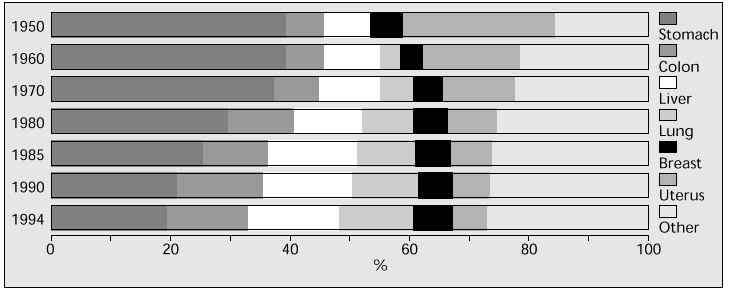
Among the so-called adult diseases, mortality from malignant neoplasms is at its highest since 1980 [7]. Some specific aspects of the change in proportion of female mortality from malignant neoplasms between 1950 and 1994 are shown in Figure 6. The proportion of mortality from stomach and uterine malignant neoplasms has decreased dramatically. Changes in life style including dietary habits and the progress of diagnostic and therapeutic methods are generally considered to be significantly responsible for these improvements. On the other hand, the increasing trends in incidence of and mortality from colon, lung and breast cancer are notable [7]. In particular, the incidences of breast cancer per 100,000 population in 1979 and 1989 were 15.1 and 27.6, respectively. The mortality rates in the same population in 1960 and 1994 were 3.5 and 11.3, respectively. The increasing trend of breast cancer is partly explained by the earlier onset of menarche and the delayed age at first birth in recent years [8]. As a specific finding in Japanese women, small declines in incidence and mortality rates from breast cancer have been observed after the menopause [9]. This age-related change in mortality/incidence pattern has rarely been observed in most Western countries, where these rates have increased with age even after the menopause. Thus, in order to explain this discrepancy between Japan and the West, it is important to conduct further studies on the relationships between genetic and environmental factors and the aetiology of breast cancer.
Fig. 6: Change in proportion of female mortality from malignant neoplasms in Japan between 1950 and 1994.
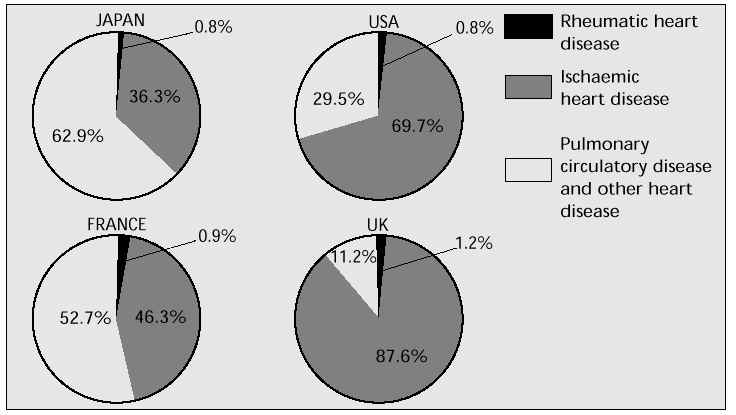
A sharp increase in mortality from heart disease has become a serious concern in Japan. The mortality rate from ischaemic heart disease was 9.9/100,000 population in 1950, whereas in 1994 it was 46.7/100,000 population (Fig. 7) [7]. It has been reported that the mortality rates of ischaemic cardiovascular disease are highest in the USA and UK, while in Japan, the mortality rates of pulmonary circulatory disease and other types of heart disease are greater than mortality from ischaemic cardiovascular disease (Fig. 8) [10]. Much epidemiological data support the view that there are clear differences in mortality from heart disease between the two sexes, especially with regard to age. In a comparison of Japanese male and female mortality rates from heart disease throughout the total life span, the net mortality rate of men was greater than that of women, but the male:female ratio declined significantly after the age of 60 and became almost identical among the elderly population. These statistics strongly suggest that Japan must urgently establish a system to prevent and manage life-threatening heart disease in the postmenopause. At the same time, they are indicative that other countries in the East Asian region will face a similar situation in the near future.
Fig. 7: Change in mortality rates from heart diseases in Japan per 100,000 population.
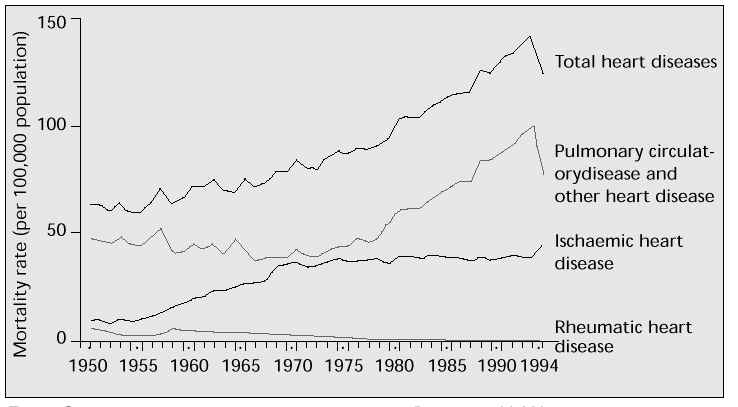
Fig. 8: Proportion of mortality rates from heart diseases in four countries in 1994.
The pattern of climacteric symptoms in the East Asian region
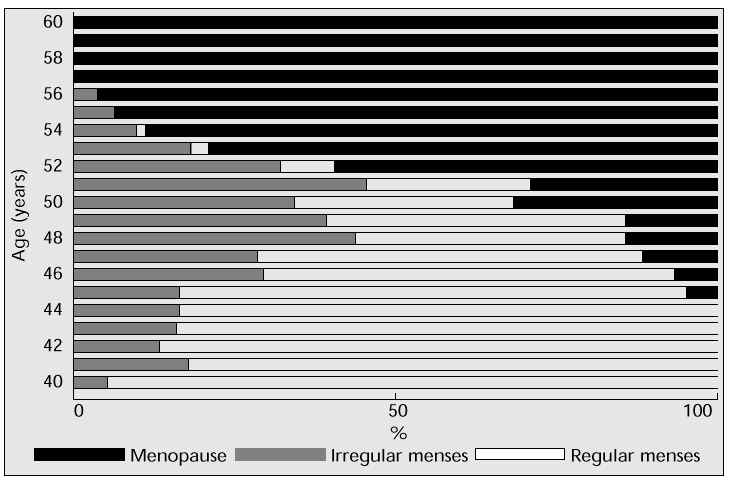
It was once assumed that the menopause was not only a universal event but that its timing and physiological implications were universally the same. However, the accumulation of global information concerning the status of women during the menopause from different parts of the world has raised questions whether women experience menopause at the same age, with the same symptoms and the same mortality, irrespective of where they live. To answer these questions, the influences of ethnic, socioeconomic and environmental factors on the events associated with the menopause have been extensively studied [11, 12]. A number of investigators have focused on the situations in particular countries of the East Asian region as counterparts to the Western world. Although there is a great heterogeneity in socioeconomic and cultural background among women living in the East Asian region, some similar and some differing aspects in the status of menopausal women have been identified. A study conducted in menopausal women in seven South-East Asian countries [12] revealed a median age at menopause of 51.09 years, which appeared to be within the range observed in Western countries. The menstrual status of Japanese women between the ages of 40 and 60 is illustrated in Figure 9. The menstrual cycles of a significant number of normally healthy women became irregular at the age of 40 and more than half of the women reported cessation of menstruation at the age of 52; all had become menopausal at the age of 57. In general, these results do not differ from the trends observed in the West. In attempting to assess the variables influencing the transition to menopause in South-East Asia, age, ethnic group and age at menarche were shown to be significant. It was suggested that a later age at menarche favoured an earlier menopause [12].
Fig. 9: Change in menstrual status in Japanese women between the age of 40 and 60 years.
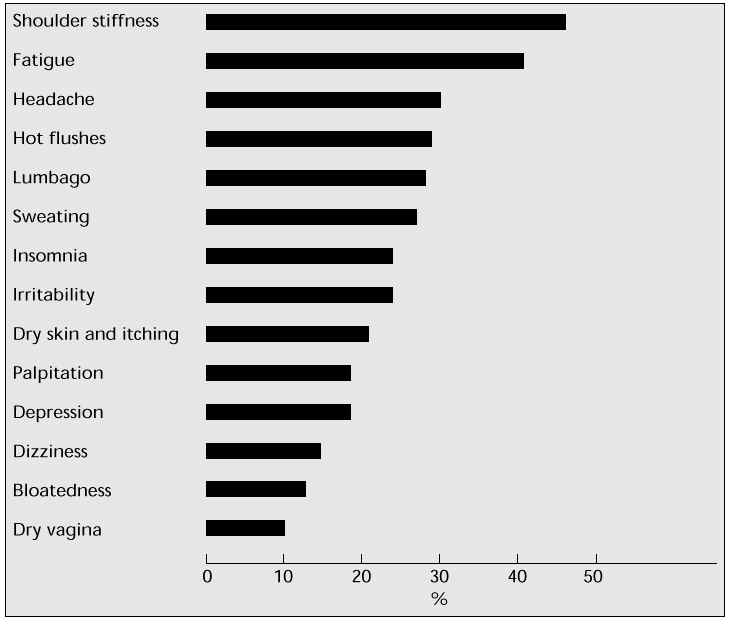
In the International Health Report [13] it was concluded that the menopause seems to be associated with fewer and less severe symptoms in Asia than in the West. However, it should be borne in mind that this conclusion was drawn from the results of a survey using a symptom list originated for European women. One could therefore speculate that most previous studies may not have been able to clearly identify the characteristics of symptoms of women living in non-European countries. Even so, it is clear that menopausal Asian women experience to a lesser extent psychological complaints such as anxiety, irritability, headache, depression, insomnia, and vasomotor complaints including hot flushes, sweating, palpitation and dizziness. A recent survey conducted by our group (to be published) covering more than 3200 healthy Japanese women between the ages of 45 and 60 revealed that shoulder stiffness is the most common complaint (45%); the percentage of women who were disturbed by severe vasomotor symptoms was approximately 25% (Fig. 10).
Fig. 10: The incidence of climacteric symptoms in Japanese women during the perimenopause.
Conclusion
Aggregate statistics strongly indicate a sharply increasing rate in the number of postmenopausal women in the East Asian region in the early part of the next century. Longevity is as much a general trend in this part of the world as it is in the developed world, and much attention will be paid to the quality of life of the postmenopausal generation of women. Specific mortality rates from so-called adult diseases have been reported in part in recent years. But in order to establish preventive strategies, the characteristics of these diseases and their precursors need to be clarified, and a survey of their incidence by age and menopausal status is needed for each country.
The prevalence of climacteric symptoms in some countries of the East Asian region has been reported, but the quantity and quality of the overall information are still far from satisfactory. In most of the studies carried out so far, climacteric symptoms were analysed using a scale which had originated in the West, without taking into consideration the socioeconomic factors and cultural background of this region. Until there are adequate data on the magnitude and extent of menopausal problems in this region, it is not possible to recommend appropriate interventions or treatments.
References
1. World Health Organization. Regional highlights: the World Health Report, 1996: fighting disease, fostering development. Geneva: WHO; 1996.
2. World Bank. World development report, 1993: investing in health. New York: Oxford University Press; 1993.
3. United Nations. Demographic yearbook, 1993. New York: United Nations, Department of International and Social Affairs; 1993.
4. Ministry of Health and Welfare. Population census of Japan. Tokyo: Statistics Bureau Management and Coordination Agency, Ministry of Health and Welfare; 1996.
5. World Health Organization. The state of world population. Geneva: WHO; 1996.
6. Aso T. Reproductive health before and after childbearing age: the Japanese scene. Adv Contracept 1996; 12: 305–8.
7. Ministry of Health and Welfare. Vital statistics. Tokyo: Statistics and Information Department, Ministry of Health and Welfare; 1996.
8. Wakai K, Suzuki S, Ohno Y et al. Epidemiology of breast cancer in Japan. Int J Epidemiol 1995; 24: 285–91.
9. Hirose K, Tajima K, Hamajima N et al. A large-scale, hospital-based case-control study of risk factors of breast cancer according to menopause status. Jpn J Cancer Res 1995; 80: 146–54.
10. World Health Organization. World health statistic annual. Geneva: WHO; 1994.
11. Lock M. Encounters with aging: mythologies of menopause in Japan and North America. Berkeley, CA: University of California Press; 1993.
12. Boulet MJ, Oddens BJ, Lehert P et al. Climacteric and menopause in seven South-East Asian countries. Maturitas 1994; 19: 157–76.
13. Payer L. International health report: menopause in various cultures. A portrait of the menopause. Carnforth: Parthenon; 1991.
14. The Studying Group of Reproduction and Endocrinology. The management of health care for the middle aged woman. Acta Obstet Gynecol Jpn 1997; 49: 1019–43.