First Consensus Meeting on Menopause in the East Asian Region
Symptoms of the menopause and their treatment
Nikorn Dusitsin
Institute of Health Research, Chulalongkorn University, Bangkok, Thailand
Vasomotor symptoms
Hot flushes and night sweats are thermoregulatory disturbances characteristic of the menopause. These symptoms are described as ‘recurrent, transient periods of flushing, sweating, and a sensation of heat, often accompanied by palpitation, feeling of anxiety, and sometimes followed by chills’ [1]. Hot flushes start as a sudden feeling of heat in the chest and then spread to the neck and face and are associated with diffuse or patchy flushing of the skin accompanied by profuse sweating. The flushes, which usually last about 3 min, are induced by vasodilatation which continues for at least 5 min after symptoms have subsided. Flushes may be induced by tension or nervousness and their frequency, duration and intensity can be reduced in some subjects with placebo interventions, although oestrogen therapy is the most effective treatment.
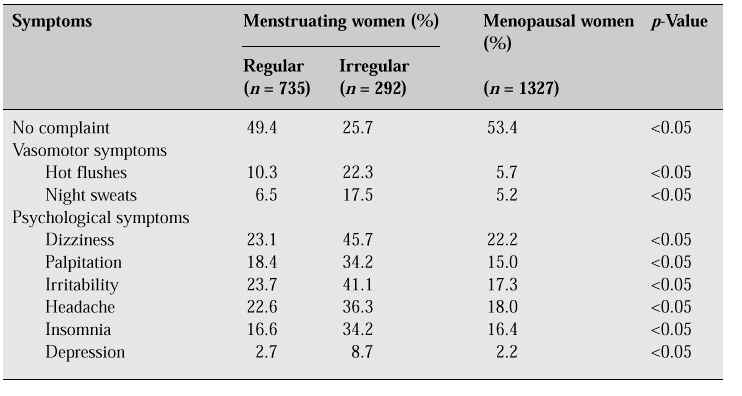
The prevalence of hot flushes associated with the menopause varies widely between different cultures and countries. The prevalence has been reported to range from 0% in Mayan women to 80% in Dutch women. In general, flushes and sweats are more common in European and North American women than in other populations. The American study noted that the peak flush rate occurred during the menopausal transition, while the Dutch study reported that the highest prevalence of hot flushes occurred in the 6–12 months after the final menstrual period [2]. In our study in Bangkok, the peak flush rate occurred during the period of menstrual disturbances prior to the final menstrual period (Table I).
Table I: Menopausal symptoms found in a study of Thai women aged 45–59 years in Bangkok [3].
Hot flushes may be more severe in women who undergo bilateral oophorectomy than in those who have a natural menopause. Hot flushes are not unique to menopausal women. A similar phenomenon has been reported in some women before the menopausal transition, and in some men.
A high intake of dietary phyto-oestrogens may play an important role in reducing the consequences of oestrogen deficiency. This has been suggested as a possible explanation not only of the lower frequency of menopausal symptoms, but also of the lower rates of breast cancer and hip fracture in Japanese compared with Caucasian women.
The role of exercise also justifies further investigation. Exercise seems to protect against depression and reduce the frequency of vasomotor symptoms [4]. Regular and proper exercise would also offset the long-term consequences of oestrogen deficiency such as osteoporosis and coronary atherosclerosis.
Treatment with oestrogens and/or progestogens reduces the frequency and severity of hot flushes. Oestrogens can be administered orally, transdermally or as implants. Oestrogens can be used with sequential progestogens, or both progestogens and oestrogens can be given continuously.
Irregular menstruation in the perimenopause
Menstrual irregularities (variable cycle length, heavier, prolonged or reduced menstrual flow) occur during the menopausal transition. While some women stop menstruating abruptly, the majority may experience months or years of menstrual disturbances before menses cease. Data on hormonal changes have shown a clear exponential decline in oestradiol during the perimenopause and a commensurate increase in follicle-stimulating hormone during the same period [2].
Other complaints
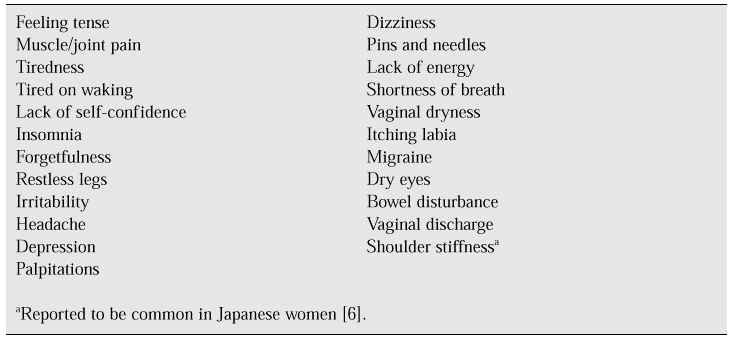
A large number of other somatic and psychological complaints are often reported by women in the climacteric (Table II).
Table II: ‘Atypical’ climacteric complaints [5, 6].
These symptoms are not specific to the menopause and are presumed to be psychological and sociocultural in origin. In several studies, occurrence of these symptoms is not highly correlated with menopausal sta-tus, but the symptoms are strongly correlated with each other. Stressful life events which are common in the mid-life period frequently precipitate a depressed mood [3]. These symptoms seem to peak during the perimenopause and decline after cessation of menstruation. Many women report symptoms while they are still having regular and presumably normal cycles (Table I).
Most of the placebo-controlled trials that have used oestrogens to suppress individual atypical symptoms have demonstrated no statistically significant benefits of this treatment [7]. The origins of these symptoms are probably multifactorial in their pathophysiology and the deficiency of oestrogens may play an important contributory or accelerating role. In clinical practice, some patients presenting with these symptoms do benefit from oestrogen supplementation. However, there is a paucity of information related to these symptoms among Asian menopausal women.
Conclusions
— The available evidence suggests that the frequency and severity of vasomotor symptoms are lower in East Asian than in Caucasian women.
— The administration of oestrogen is effective in controlling vasomotor symptoms in East Asian women.
— Further data are needed to clarify the nature and frequency of menopausal symptoms in East Asian women.
References
1. Kronenberg F. Hot flashes: epidemiology and physiology. Ann N Y Acad Sci 1990; 592: 52–86.
2. McKinlay SM. The normal menopause transition: an overview. Maturitas 1996; 23: 137–45.
3. Chompootweep S, Tankeyoon K, Yamarat K, Poomsuwan P, Dusitsin N. The menopausal age and climacteric complaints in Thai women in Bangkok. Maturitas 1993; 17: 63–71.
4. Hammar M, Berg G, Lindgren R. Prevalence of hot flushes among postmenopausal women taking regular exercise [abstract 246]. Data presented at the 6th World Congress on the Menopause, Bangkok, 1990.
5. Rekers H. Mastering the menopause. In: Burger H, Boulet M, eds. A portrait of the menopause: expert reports on medical and therapeutic strategies for the 1990s. Carnforth, UK: Parthenon, 1991; 23–43.
6. Aso T. Demography of the menopause and pattern of climacteric symptoms in the East Asian Region. This volume.
7. World Health Organization. Research on the menopause in the 1990s. WHO Tech Rep Ser 1996; 866.